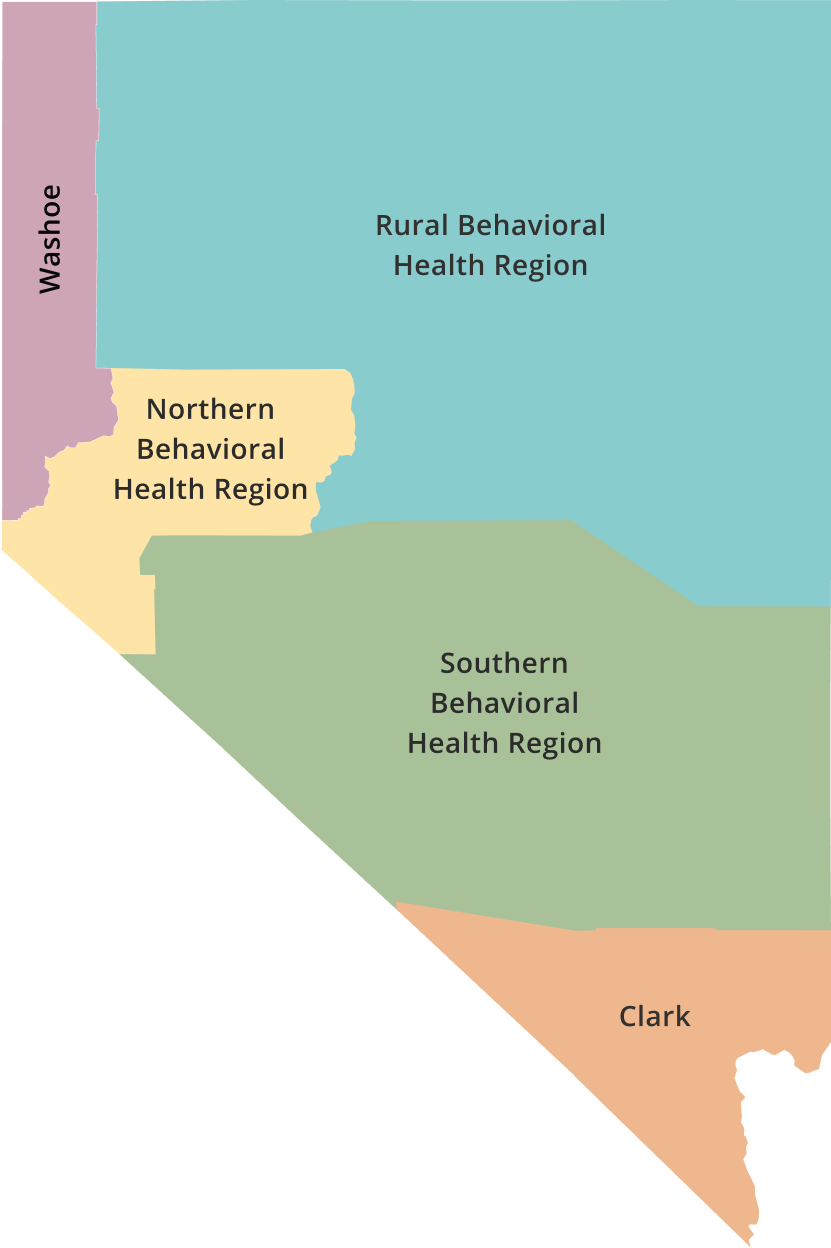
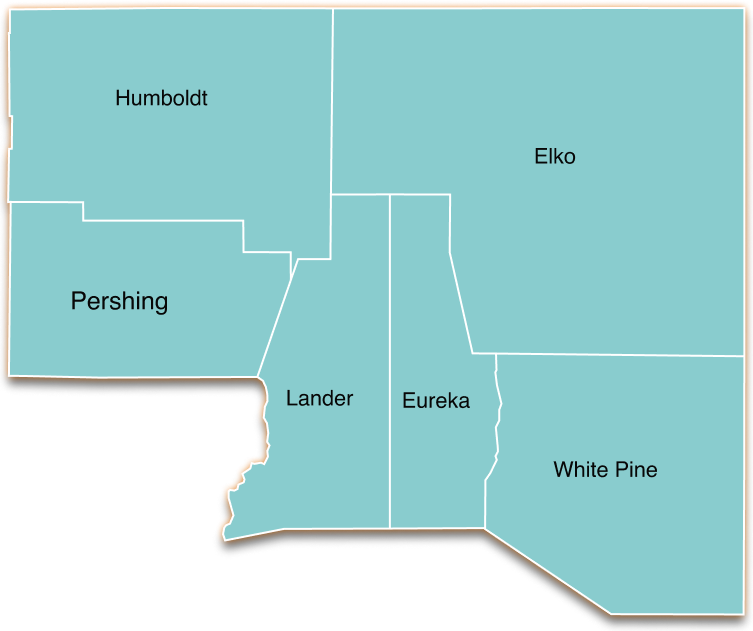
Southern Behavioral Health Region
This unique southern rural region consists of Mineral, Lincoln, Esmeralda, and northern Nye counties, stretching across approximately 28,000 square miles in southern rural Nevada. When southern Nye County is included, the estimated population is 55,990 according to some sources listed. The total population for the actual southern behavioral health region, which does not include southern Nye County, is approximately 16,000, so this illustrates that southern Nye County including the town of Pahrump (in the Clark County Behavioral Region) holds most of the population in southern rural and frontier Nevada, especially in Nye County. When you include all of Nye County, the southern region’s population is approximately 62,999. Lincoln County borders Clark County which is to the south as well as Utah to the east and Arizona to the southeast. Nye County, the largest geographic and most populated county in this region, has California on the southwestern border and sits in the middle bordering Lincoln to the east and Esmeralda and Mineral to the southwest and west, respectively. Mineral and Esmeralda Counties are southwestern border counties connecting with California as well.
According to the 2024 Southern Epi Report, “White non-Hispanic comprises 75.8% of Southern Region’s population, followed by Hispanic (15.7%), American Indian/Alaska Native non-Hispanic (3.1%), Black non-Hispanic (3.1%), and Asian/Pacific Islander non-Hispanic (2.3%). The population consists of approximately equal percentages of males and females.”
Three tribal communities reside in or near the southern region: Duckwater Shoshone – https://duckwatertribe.org/ ; Shoshone Yomba Tribe – Yomba Tribe; Walker River Paiute Tribe – https://www.wrpt.org/.
Southern Regional Behavioral Health Resource Guide (2023-2024) Online Version
Demographics and Geography
| County | Seat | Population | Area |
| Esmeralda | Goldfield | 729 | 3,589 sq mi |
| Mineral | Hawthorne | 4,475 | 3,757 sq mi |
| Nye – northern | Tonopah – north Nye | 6,000 approx. | 9,737 sq mi approx. |
| Lincoln | Pioche | 4,345 | 10,635 sq mi |
Members serving on the Southern Regional Behavioral Health Policy Board are community leaders, law enforcement, healthcare and treatment providers, family and peer advocates, and more. They bring diverse perspectives to the Board and are passionate about collaborating to improve the behavioral health system in the Southern Region. The board resumed meeting in June of 2023. The Board along with regional stakeholders and county behavioral health task groups and coalitions continue to develop a shared understanding of the behavioral health issues facing the region. The Southern Regional BH Policy Board has begun to learn more about the roles and responsibilities in addition to the connection to the Coordinator role and work. Shared goals are emerging in conjunction with local, regional, and state partners to identify and align priorities and solutions whenever possible. Through ongoing discussion and work, the SRBHPB members, shown below, will continue to examine the needs (gaps and barriers) and strengths and highlights to establish priorities and recommendations for the coming year(s). The most recent legislative initiative sponsored by the policy board is AB31 supporting Non-Emergency Secure Behavioral Health Transportation.
https://www.leg.state.nv.us/App/NELIS/REL/83rd2025/Bill/11803/Exhibits
Board Members
- Chair: Dr. Kevin Osten-Garner, PsyD, Founder and Principal Advisor, Osten-Garner Advisory
- Vice Chair: Stacy Smith, CEO, NyE Communities Coalition
- Boonn Hem, Certified Peer Recovery Support Specialist, Substance Misuse Specialist, CHW-I, Nye Communities Coalition
- Assemblyman Gregory Hafen II, Legislator/ District 36
- Missie Rowe, CEO/Administrator, Grover C. Dils Medical Center
- Scott Lewis, Director of Nye County Emergency Management; Fire Chief, Pahrump Fire & Rescue
- Sarah Dillard, Rural Program Director, Community Chest Inc.
- Whitney Koch Owens, PsyD, Owner, The Evidence Based Practice of Nevada, PLLC
- Coleen Lawrence, MSSL, EJD, President-Executive Director, Moxy Up
- Brenda O’Neil, Health Manager, Duckwater Shoshone Tribe
Positions to Fill
- Representative of the criminal justice system.” NRS 433.429 Section 3, subsection (3) – https://www.leg.state.nv.us/nrs/NRS-433.html#NRS433Sec429
- Representative of residential treatment facility, transitional housing or other housing program serving persons with mental illness or who abuse alcohol or drugs. Section 3, subsection 8(b).
- Senate Majority Leader appoints a “representative of law enforcement, with knowledge & experience with persons needing behavioral health services, Section 3, subsection (4) – Link.
Overview of Board Role/Function/Duties
- Advise the State on Needs, Issues, Gaps, and Priorities
- Note Issues with Laws and Regulations and Make Recommendations
- Information, Resources, and Service Delivery
- Coordination and Improvements in Behavioral Health
- Track-Compile Data and Outcomes / Reporting and Repository
- Reporting to the State and Commission
- Bill Draft Request and Legislation
Regional Assets, Strengths, and Highlights
- Two critical access hospitals in this rural region are significant partners and resources for the counties and the Mt. Grant General Hospital in Hawthorne provides primary care and emergency medical services in Mineral County for the surrounding area. The facility also provides inpatient care, emergency services, and diagnostic services, according to their website. They also run a skilled nursing facility and have local clinics nearby. Grover C. Dils Medical Center in Caliente (Lincoln County) also serves the region. They provide healthcare services and list a clinic in Alamo as well. They provide primary and emergency care with long-term care, and there are health clinics nearby.
- Tonopah has a free-standing health clinic run by a private provider. Although there is a “hospital group” meeting in Tonopah, there is currently no hospital in northern Nye County. Bordering Tonopah, Esmeralda County, has no medical providers other than EMS and First Responders and periodic immunization clinics. Esmeralda County government does provide resources on a commodities day on a regular basis.
- Desert View Hospital in Pahrump is outside the southern rural region but in southern Nye County and serves part of the region.
- Three of the four counties have a behavioral health task group, coalition and/or mental or behavioral health committees.
- Significant strengths lie in the resolute and creative work of the individuals, coalitions, and other agencies that have a positive impact on the region including outreach and collaboration.
- Deflection and diversion work in the southern rural region is an ongoing and significant part of the scope and work in the community and the coordinator scope of work: a MOST Team in Nye County operates out of the coalition; Lincoln County has a Most Team and Mineral County has a robust group of stakeholders that work together with law enforcement to intervene and support justice-involved individuals. Esmeralda County does not have formalized collaborative groups, but the county government, law enforcement, justice, and schools come together around significant and positive work in the community.
- The increasing presence of private providers and other non-profit agencies continue to expand to support the region virtually through in-person or hybrid/telehealth services. Many of these services are expected to be expanded statewide this coming year with the Managed Care and 988 Crisis Support Projects.
- Several tribes run health clinics and provide behavioral health work in the region: Walker River Paiute Tribe in Schurz, Nevada. The Duckwater Shoshone Tribe also runs a health clinic among other behavioral health services.
- This coordinator started a regional networking group monthly for peers, prevention substance use-misuse specialists, community health workers, and other staff to meet for support around their work in the region. A major focus has been supporting peers in health and wellness, stress and burnout, and self-care. The support was discontinued due to low attendance and the legislative session with hopes of restarting the support in the coming year.
Significant Regional Needs: Barriers and Gaps
- Notable general lack of services for both youth and elderly populations, especially awareness or knowledge of state programs across entire region. The work of 2023 included the development of the first behavioral health resource guide for the region which also included a comprehensive This guide and the distribution to over 100 stakeholders has been instrumental in meeting those needs and filling those gaps to help reduce the barriers. That resource guide needs to be updated and put online electronically. 211 and the emerging enhancement of 988 programs are also significant resources along with state and local resources guides.
- Obviously, citizens in the southern region also utilize agencies and resources in the more urban areas of Clark and Washoe and surrounding counties and states as needed and when travel and transportation are available and feasible, yet the scarcity of resources and providers create a need to travel out of the region to access specialists in healthcare, more intensive behavioral health treatment, crisis support and stabilization, and other services. Transportation complexities and scarcities around accessing medical services and healthcare and mental health crisis transport all create major barriers. On the other hand, the state has contracted with a new vendor to provide medical transport around the state and MCO’s and other providers are starting to look at ways to provide transportation and some vendors have mobile clinics.
- Although increased services around telehealth crisis and healthcare have broken down some barriers, there is still a need to connect these services with continuity of in-person care and continued development of on-the-ground care and services for those who have more serious ongoing needs and for transition in conjunction with telehealth. Developing and enhancing the infrastructure for reliable telehealth is also an ongoing need and often a major barrier.
- Coordinated behavioral health crisis response and stabilization are also ongoing needs. Although some parts of the region have a more developed response in this area, training and crisis planning needs continual development, coordination, and training that can support the region including supportive telehealth options. Some rural areas are also facing shortages of volunteer emergency personnel and first responders.
- Although the concept of diversion and deflection has been a priority for the state and this coordinator, no new funding has been received to start or enhance deflection and diversion in the southern rural region. Although some areas have more fully implemented deflection and diversion, there is a need for developing and enhancing these community-and-jail-based initiatives around multi-disciplinary sectors; moreover, barriers with workforce, buy-in, resources, funding, and collaboration make this even more challenging.
- Lack of healthcare and behavioral health workforce across the southern region that includes recruitment, retention, and training of professionals also creates major concerns and are ongoing issues and priorities around the state.
- Need for improved access to behavioral health supportive housing and in-patient (residential) treatment for Serious Mental Illness (SMI), Opioid Use Disorder (OUD), and substance use disorder (SUD) as well as services to expand Medication Assisted Treatment (MAT) in jails and outpatient clinics. Long waits for evaluations and intensive residential care are barriers to access. Sometimes patients must stay in local rural hospitals who are not equipped for behavioral health support while the patients wait for evaluation and admission or transport to other facilities outside the region.
- Substance use-misuse and the need for increased prevention, educational programs, treatment and coordinated Some counties (schools and coalitions) do have grants, funding, and agency programming around these areas, but more is needed in other counties and sustainability in other areas. The extension office and other youth serving agencies do have a significant presence in the region, but these services are often not enough.
- Housing and Homelessness: shortage and cost of housing are significant issues statewide, especially in rural, frontier, and tribal areas where land may be available but resources to build or remodel homes are scarce. The exact nature or scope of homelessness in rural and frontier areas is difficult to determine for several reasons. Homelessness looks different than in urban areas. In rural areas, people who have housing issues often live in RVs in outlying areas, often off the grid and without electricity and running water. Homelessness often consists of multiple families or individuals living with others in a more transient nature, and this often goes underreported.
- Increased education and training around peer recovery, stigma, reducing death and overdose, crisis intervention (CIT), emergency services, and other behavioral health areas are ongoing needs.
- Ongoing data gaps and barriers provide persistent challenges in collecting granular rural data for both behavioral health and overdose surveillance.
Transportation and Transport
- No significant public transportation services exist in the southern RBH region.
- Individuals and families travel long distances for work or more specialized care.
- Taking time off for work and school, if it is even possible, creates issues. Travelling long distances to urban areas for shopping and services also creates issues with financial concerns, including possible need for overnight lodging, extra fuel, meals, and other costs including childcare or other family care.
- Potential increased health risks for those traveling in vehicles with poorly performing or inadequate air conditioning in the summer months on the long commutes to secure health care services in urban areas.
- Two of four counties and some smaller communities and tribes have no hospital, emergency, and/or shopping/groceries nearby (50 plus miles).
- Agency (law enforcement/EMS) transport residents to access general medical care, specialized services, and mental health crisis or residential/inpatient treatment.
- Traveling long distances (out-of-county) requires personnel to be out-of-service or unavailable, even when understaffed, and sometimes paid overtime, which affects already constrained budgets.
- A declining volunteer workforce for emergency services that exacerbates EMS systems in rural and urban counties. Volunteers may not have training on how to safely transport someone with a behavioral health problem in crisis as much as highly trained, certified staff in BH crisis transport.
The Southern Regional Behavioral Health Policy Board resumed operations in June 2023. The following information aligns with current state and regional goals and objectives as well as information taken from the 2022-2025 Annual Reports. The coordinator and the board continue working together and with local and regional stakeholders to develop initiatives around local and regional needs and priorities. The SRBHPB will begin reviewing these and/or developing other priorities and initiatives in the coming year(s). In the Legislative Session of 2025, the policy board sponsored AB31: https://www.leg.state.nv.us/App/NELIS/REL/83rd2025/Bill/11803/Overview. The bill did not pass.
Three of the primary content areas the board will be working on are as follows: substance use/misuse prevention; mental health; and opioid response.
Overview of Priorities and Strategies
- Continue understanding local and regional highlights and strengths, opportunities, and needs (gaps and barriers).
- Continuing to develop strategies, priorities, and initiatives as they relate to the southern rural and frontier region and statewide behavioral health.
- Implementing a direct impact and sustainable culture of concrete action and communication leading to tangible results (effective execution and follow-up).
- Tiered Process based upon demographics (population thresholds) and nearby infrastructure in relation to various parts of the region
- Developing and implementing outreach and education for the public and stakeholders.
Outreach and Education (inform/educate board/public)
- Involving “public voice” and community stakeholders and partners.
- Reducing barriers to public input and involvement.
- Value-added benefit of a policy board for the public
- More accessibility – social media to collect feedback to inform and educate the public.
- Earning public trust and communications to demonstrate how board makes a difference.
- Ways to remove barriers and increasing presence in the communities.
- Provided updates at behavioral health and other community groups about policy board.
- Examen historical context, communication, trust, and feedback issues, and impact in communities before moving into policy.
Ongoing Issues
Transportation and Transport: Medical, Behavioral or Crisis
- Resources and funding for rural outreach – infrastructure – creative options
- Factors: reducing barriers of high caseloads, short staffing, large geographic distance in regions, and scarce services and limited resources and allocation; safety as a factor.
- Availability of facilities issues in relation to transport – priority levels dictate urgency / access to hospitals, residential services, and facilities.
- Summary of Process: “Medical necessity” – sheriff-EMS transport variables – lack of consistency in transport services – different protocols and procedures for each county- driven by medical necessity that drives reimbursement and levels of services – physical-medical treatment vs. emotional and behavioral health issue or both / fee for service and other payment issues and barriers – reimbursement and payment as restrictions or avenues to service and transport. Depends on where patient is originating from, and issue of mental health crisis holds (3-day) – decision for transport – responsibility for payment and sheriff or ambulance transport
- Workforce and Staffing (hospitals, law enforcement, EMS, clinical, peers, CHWs): ,
- Boomerang effect: high utilizing patients that continually cycle through the system
Crisis Response and Stabilization: rural and frontier – hospitals, facilities, and community.
- Improve the capacity of local hospitals – addressing reimbursement services – noted overlap in transportation and transport above. Different options for transport.
- Barriers and access to services – high risk factors
- Discharge and transition planning and services – movement between levels
- Stabilization and Treatment: establishing more outpatient care
- Some areas do not have hospitals: telehealth and limited onsite services
- Partnerships and creative collaboration are essential: local, regional resources & agencies.
- Intake and assessment – earlier intervention – levels of care determined.
- Local options – community-based options and short-term stabilization
- Communication – utilization of local resources – meeting individuals where they are
- Homelessness issue and difficulty with date and reporting
- Prevention level services – upstream funding and programs
Access to Care and Services: barriers to insurance and care and other related issues
- Any willing provider, paneling of providers / access issue – inaccuracy, not accepting patients, barriers – contributes to scarcity of providers.
- Telehealth (virtual): limited or short-term solution vs. value of in-person care.
Training and education: crisis response, mental health, substance use-misuse, opioids, naloxone, Narcan, first responder-EMS, law enforcement. This relates to and supports other issues.
Youth, parenting support, family systems, and engagement: residential and community support and transition. Service complexities with guardianship concerns and funding.
Workforce Development (GOED): Community Health Workers, Peer Specialists, Clinical Staff, Certifications, and Licensing. This issue is related to barriers and access to care, transport, and crisis.
Courts and justice: specialty courts, mental health, deflection, and diversion
Data assessment and collection as a guiding focus: collection and reporting – issues, availability, barriers, and complexity. This issue is related to all other issues and cuts across lines.
Regional Update – Spring 2025
The region has four counties spanning an area larger than West Virginia and a total population of less than 16,000.
Significant assets and strengths in the region include:
- Creative, hard-working, and resourceful individuals.
- Community coalitions and agencies serving the region.
- Deflection & Diversion programs to link people to evidence-based care and services instead of incarceration have been launched but are limited with growth challenges.
- Specialty Courts, Judicial, Legal, and Probation are regionalized.
- Multi-Disciplinary Team(s) and Behavioral Health Groups/Committees are established.
- Robust collaboration, communication, and services.
- Hospitals, schools, tribal, family, senior, and youth services/programs.
Primary gaps and barriers are:
- Scarcity of behavioral health clinical services and providers in the region.
- Difficulty in recruiting and retaining workforce in rural areas.
- Lack of behavioral health supportive housing/residential services/treatment.
- Long waits for evaluations and intensive residential care access.
- Reliance on community health workers due to lack of adequate clinical support.
- Scarcity and under-utilization of peer support.
Recent Developments
- Developed and distributed regional resource guides, available at https://nvbh.org/wp-content/uploads/2023/09/SouthernRegionResourceGuide.pdf.
- County Community Needs Assessments and Opioid Plans have been completed by Esmeralda, Mineral, and Nye Counties with Lincoln starting the process.
- Three of the four counties have either implemented or started the process for the Virtual Community Care (VCC) Program (Avel Tablet Program) for crisis-related telehealth support in partnership with law enforcement.
- Support of Mineral County Behavioral Health Task Group, Coalitions, and Tribes.
- Regional support of Community Health Workers and peer networking.
- Naloxone training support and harm reduction-opioid kit distribution.
- Support of the Youth Experiencing Homelessness Study (2023-2025); information at https://www.socialent.com/youth-experiencing-homelessness-study-2023-2025.
- Participation in the Community Inclusion Peer Support Project with national and statewide connections; see https://copelandcenter.com/training/peer-supported-community-inclusion.
Current Activities
- Support behavioral health clinical services and Mental Health Committees.
- Enhance Deflection & Diversion programs.
- Ongoing Suicide Prevention Training but need for Crisis Intervention Training (CIT) with support and follow-up.
- Address long waits for evaluations and long distances to intensive services through identifying behavioral health transportation alternatives.
- Support community health workers with substantial clinical support, and develop under-utilization of peer support.
- Review and support projects to assess, develop, and integrate emergency planning, public health, and behavioral health.
Upcoming Priorities and Plans
- Expanding telehealth and connecting with enhanced in-person care.
- Need for increased education and training around stigma, harm reduction, suicide, and crisis intervention (CIT).
- Enhance data assessment, collection, and reporting: issues, availability, barriers, and complexity.
- Support and expand harm reduction with opioid overdose prevention programs, Narcan training, and other strategies.
- Invest in recruitment, training, and retention programs for clinical and non-clinical professionals.
- Support for 988 Crisis Support and Stabilization
Historical Context (2023-2025)
The coordinator and the board work together each year to collaborate with local and regional stakeholders and state partners to develop strategies and recommendations around local and regional needs and priorities. Initial strategies and recommendations are as follows:
General Recommendations and Strategies
- Regular updates and distribution of the Southern Regional Behavioral Health Resource Guide (2023-2024). Increasing knowledge and support around statewide and community programs and resources which includes updating local and regional behavioral health resource guides keeping up with local providers and resources that connect with regional and statewide support. These local and regional guides could be connected to statewide initiatives around 211 and 988: links and mapping; electronic and mobile access; regular updates with grassroots agency input as changes occur in real-time, and connection between regions, urban areas, in a multi-disciplinary fashion.
- Ongoing networking, collaboration, and relationship building with NRHP, NPHF, policy boards, hospitals, providers, government and law enforcement agencies, and other local/regional/state/ tribal stakeholders and partners. This includes ongoing support of coalitions, behavioral health committees, and groups.
- Increase in data and resource review and collection to support collection, management, analysis, and reporting
- Ongoing updates and review of strengths, needs, opportunities, barriers, and gaps.
- Strategies, priorities, and recommendations on evidence-based models using action planning and collaborative systems for implementation and sustainability.
- Support and advocacy for increased funding, resources, staffing, technical assistance and training for the southern region.
- Continued improvement in linkage and liaison work between the community, board, and state including evaluation of efforts, perspectives on the state-local relationship for improvement, and quantitative and qualitative measurements connected to outcomes.
- Ongoing enhancement of behavioral health coordination in the southern region including mental health, opioid response, and substance use-misuse prevention and social determinants of health and wellbeing.
Regional/Statewide Recommendations and Priorities
- Continue building relationships with behavioral health agencies, local and regional law enforcement, courts, and judicial staff including specialty courts.
- Ongoing collaboration and networking between and among coordinators in rural and urban areas as well as policy and other boards, and multi-disciplinary local and state agencies.
- Increasing access to care and reducing barriers at all treatment
- Renewing the focus on transportation includes decreasing barriers to accessing long distance care by building upon local resources, using existing and creative intervention as well as securing funding for necessary transportation and crisis transport around behavioral health.
- Review the concerns and needs of the behavioral health workforce and work with local, regional, and state individuals and entities around retention, training, and support if
- Support the development and implementation of effective and efficient use of telehealth and virtual services by supporting and connecting in-person, on-the-ground services in the region as it relates to transportation.
- Examine the roles of community health workers and peer specialists and enhance the workforce and development in those sectors.
- Continue advocating for supportive housing as well as state and national models around housing and homelessness in rural areas. This will include a review of social determinants of health and how they relate to housing and homeless needs and concerns. Increased and enhanced reporting followed by increased access to housing. Review, survey, and examine how supportive housing can be aligned with best practices for residents with behavioral health issues in the region. This could include developing living room models or peer respite homes.
- Review existing regional crisis response systems including the need for, and support of, developing or expanding those services and training in the region. This includes serious collaboration with the statewide 988 Crisis Support initiative and the MCO rollout in 2026.
- Review and adapt existing crisis intervention, response, stabilization in other regions and states and bring new strategies for southern rural, frontier, and tribal areas.
- Continue evaluating existing and emerging deflection and diversion and programs like MOST and FASTT and support funding and expansion for counties in the southern region.
- Aid individuals, agencies, and communities by providing resources, training, and technical
- Enhance strategies and resources around reducing death and overdoes from substance misuse including opioids. Supporting coalitions and agencies with training on Narcan as well as Naloxone distribution.
A Southern Regional Behavioral Health Resource Guide (2023-2024) is in process to print and will be officially published and distributed both hard copy and electronically in August-September of 2023. A preliminary version of the guide can be found below and on the Publications and Reports section of this website on the following page
Southern Regional Behavioral Health Resource Guide (2023-2024) – Online Version
Southern Regional Resource Appendix: https://nvbh.org/pdf-preview?id=4963
Nevada Opioid Center of Excellence: Overdose Data to Action Program (OD2A) – https://nvopioidresponse.org/initiatives/od2a/
Regional Resources
Community Chest: https://communitychestnevada.net/
Nye County
Nye County Communities Coalition: https://nyecc.org/
Resource Directory – 2022-2024 (see Southern Region Documents and Publications)
Food Pantry List – 2023 (see Southern Region Documents and Publications)
Lincoln County
Lincoln County Coalition: https://lccoalition.org/
Mineral County
Mineral County Resources – see Southern Region Documents and Publications
Esmeralda County
Senior Transportation (Goldfield)
- Director Maureen Glennen
- Email: mglennen@esmeraldacountynv.org
- Clerk Email: ncolunga@esmeraldacountynv.org
- Address: 403 W. Crook Ave, Courthouse, 2nd Floor; Goldfield, NV 89013 / Phone: 775-485-3406
- Website: https://www.accessesmeralda.com/county_offices/senior_transportation.php
Commodities
This resource in Esmeralda County is a joint effort with 3 Square of Las Vegas. The resource includes two deliveries of food including frozen and fresh: fruits, vegetables, meats, canned & boxed goods. This food is distributed to volunteers of the other unincorporated towns (Gold Point, Silver Peak, and Fish Lake Valley, and then the food is delivered to local families. The distribution happens the first Wednesday and third Monday (barring holidays). Anyone who meets the income requirements may contact the Commissioner’s Office for an application and times for distribution in their area.
Pickup Locations
- Goldfield: Commodities Barn on Euclid across from the Fire Barn (Noon-1:00 pm)
- Fish Lake Valley: Community Center (2:15 to 3:15 pm)
- Silver Peak: Library (11:00 to 12:00 pm)
- Gold Point: Delivers to the 6 residents there as soon as she gets back to Gold Point (10-10:30 am)
State and National Resources and Data/Documents
- DHS Office of Analytics: https://www.dhs.nv.gov/Programs/dhhs-office-of-analytics/
- Data and Reports: https://www.dhs.nv.gov/Programs/dhhs-office-of-analytics/office-of-analytics-data-reports/
- Regional Behavioral Health Policy Board data dashboard at https://nvbh.org/dashboard//.
- Nevada Rural Hospital Partners Reporting and Data: https://data.nrhp.org/
- Behavioral Health Epidemiologic Profile 2024: Southern Region, Nevada: https://www.dhs.nv.gov/siteassets/content/programs/office-of-analytics/2024_Southern_Region_Epidemiologic_Profile_2.pdf
- Nevada Youth Risk Behavior Surveillance System (2023): https://scholarwolf.unr.edu/communities/e6a2e31a-f60e-4ead-b7f6-fc806ecd0ff7
- Nevada Rural and Frontier Health Data Book (2025): https://www.nvpca.org/nevada-rural-frontier-health-data-book
- Nevada Overdose Data to Action Program (Opioids): https://nvopioidresponse.org/initiatives/od2a/
- Southern Region Annual Report (2022): https://nvbh.org/pdf-preview?id=4857
- Coordinator’s Final Report, September 2023 Final: https://nvbh.org/pdf-preview/?id=5253
- Southern Region Annual Report (2023): https://nvbh.org/pdf-preview/?id=5251
- Coordinator’s Report, September 2025: https://nvbh.org/pdf-preview/?id=5587
- Annual Summary (July 2024): https://nvbh.org/pdf-preview/?id=5254
- 2025 Legislative Overview: https://nvbh.org/pdf-preview/?id=5541
- Southern Region Scope of Work: FY 23
- Southern Region Scope of Work: FY24
- Southern Region Scope of Work: FY25
Nevada 211: https://www.nevada211.org/
Nevada Recovery Resource Hub: https://forrecovery.org/resources/
NAMI
Warmline: https://namiwesternnevada.org/resources/nevada-warmline/
Caring Contacts: https://namiwesternnevada.org/resources/nevada-caring-contacts/
Click to select Behavioral Health Region
Health Region
Health Region
Health Region
Health Region
Health Region
july, 2026
New Documents
| Title | Content | Date | Categories | Link |
|---|
Contact
 Nevada Public Health Foundation
Nevada Public Health Foundation